Assays of Therapy by Means of Staphylococcal Bacteriophage
By B. Bruynoghe and J. Maisin.
We have had the opportunity to use the Staphylococcal Bacteriophage for therapeutic purposes, and the few favorable results obtained encourage us to report them. This assay seemed quite logical to us, given that these bacteriolysates contain a principle immediately harmful to Staphylococci. They also contain the staphylococcal antigen essential for any active vaccination, whose therapeutic effects cannot manifest until 5 or 6 days later.
In our previous note, we saw that normal Rabbit serum does not in any way prevent the Bacteriophage from dissolving these microbes. We have also been able to confirm this fact for human serum. For this purpose, we inoculate tubes of sterile serum, on one side with Staphylococci, and on the other side with Bacteriophage and Staphylococci: the inhibition of the latter’s development occurs as it does in broth cultures. The same is true for the dissolution assays of these cultures that have already developed at the moment of the Bacteriophage addition.
Clinical Application and Results
This is not the place to give clinical details concerning the patients we have treated. We are content to report that we applied this therapy to 6 patients suffering from anthrax or furuncles (boils).
We injected doses of bacteriolysates (sterilized by one hour of heating at 56° C or 132.8° F) varying from 0.5 to 2 c.c. as close as possible to the affected region. The effect was not long in manifesting itself by the diminution of the swelling at the lesions and often by the total disappearance of the latter in 24 to 48 hours. Infections that had already reached suppuration (puss formation) empty and dry rapidly.
Following these inoculations, a feverish rise in temperature occurs in some patients; in others, the temperature hardly changes. It seemed to us that this rise in temperature occurs especially in those with vast lesions, where the rapid lysis leads to the resorption of large quantities of microbial products. The injection site is painful and slightly swollen for 24 hours.
Conclusion
We have tried this therapy in patients with anthrax or furuncles, but it’s not impossible that other lesions such as acne and the various staphylococcal complications of other skin conditions could benefit from the same medication.
These observations are obviously not numerous enough to definitively establish the value of this method. They have also not been prolonged enough to determine to what extent these inoculations protect against relapse.
(Institute of Bacteriology of the University of Louvain)
—
Essais de thérapeutique au moyen du Bactériophage du Staphylocoque,
par B. Bruynoghe et J. Maisin.
Nous avons eu l’occasion d’utiliser le Bactériophage du Staphylocoque dans un but thérapeutique et les quelques résultats favorables obtenus nous engagent à les signaler.
Cet essai nous semblait assez logique, étant donné que ces bactériolysats contiennent un principe immédiatement nuisible aux Staphylocoques et l’antigène staphylococcique indispensable à toute vaccination active dont les effets thérapeutiques ne peuvent se manifester que 5 ou 6 jours plus tard.
Dans notre note précédente nous avons vu que le sérum normal du Lapin n’empêche nullement le Bactériophage d’opérer la dissolution de ces microbes. Nous avons pu contrôler également ce fait pour le sérum humain. Dans ce but nous ensemençons des tubes de sérum stérile, d’un côté avec du Staphylocoque, d’un autre côté avec du Bactériophage et du Staphylocoque : l’inhibition sur le développement de ce dernier s’opère comme dans les cultures en bouillon. Il en est de môme pour les essais de dissolution de ces cultures déjà développées au moment de l’addition du Bactériophage.
Ce n’est pas ici la place de donner des détails cliniques concernant les malades que nous avons traités et nous nous contentons de signaler que nous avons appliqué cette thérapeutique chez 6 patients atteints d’anthrax ou de furoncles. Nous avons injecté aussi près que possible de la région malade, des doses de bactériolysats (stérilisées par une heure de chauffage à 56°) variant de 0,5 à 2 c.c. L’effet n’a pas tardé à se manifester par la diminution de l’empâtement au niveau des lésions et souvent par la disparition totale de ces dernières en a/j à 48 heures. Les infections déjà arrivées à la suppuration se vident et sèchent rapidement.
A la suite de ces inoculations, il se produit, chez certains malades, une ascension fébrile, chez d’autres la température ne subit guère de modification. Il nous a semblé que cette élévation de la température se produit surtout chez ceux atteints de vastes lésions et où la lyse rapide entraîne la résorption de grandes quantités de produits microbiens. L’endroit d’injection est durant 24 heures douloureux et légèrement œdématié.
Nous avons essayé cette thérapeutique chez des patients atteints d’anthrax ou de furoncles, mais il n’est pas impossible que d’autres lésions telles que les acmés et les diverses complications staphylococciques d’autres affections cutanées ne puissent profiter de la même médication.
Ces observations ne sont évidemment pas assez nombreuses pour établir définitivement la valeur de cette méthode et elles n’ont pu être assez prolongées pour déterminer jusqu’à quel point ces inoculations protègent contre les rechutes.
(Institut de bactériologie de l’Université de Louvain).
The article was scanned and OCRed using French as the recognition language. The OCRed text was then corrected as needed (as shown in gray). The corrected text was then translated by Claude.ai, which prior to that point was not involved in the effort. Claude.ai was then asked to generate an abstract-style narrative summary (which was then corrected manually as appropriate) and then an assessment of precedence that might be claimed by the work.
Summary by Claude.ai:
This research by R. Appelmans investigated the fate of bacteriophage in animal organisms as part of studies on its therapeutic value. Using guinea pigs and mice, the authors examined bacteriophage behavior following both oral and injectable administration, employing a functional detection method in which organ samples or excreta were added to broth, heated to 56°C to inactivate bacteria while preserving phage, then inoculated with susceptible microbes to detect growth inhibition.
When bacteriophage mixed with bread was given orally to animals, the bacteriophages appeared regularly in feces for several days, persisting longer when susceptible gut microbes were present for it to parasitize. The phage’s resistance to acids and enzymes explained its survival through the digestive tract. However, examination of internal organs revealed no bacteriophage penetration across the intestinal mucosa, a finding the authors attributed to the principle’s inability to dialyze, suggesting it could not pass through biological membranes.
In contrast, injected bacteriophage rapidly entered the bloodstream in accordance with earlier findings by Bordet and Ciuca. However, its presence in blood was brief, as it was progressively eliminated through the kidneys and intestines, disappearing completely within 24 to 48 hours depending on dose, with no traces detected after five days. Notably, the spleen retained substantial quantities of bacteriophage even when it had been cleared from other organs, a phenomenon the authors connected to the spleen’s known role in retaining microbes during infections. This splenic persistence was temporary; after fifteen days, no bacteriophage remained, which the authors attributed to neutralization by antibacteriophage antibodies that form in the organism, as demonstrated by Bordet, Ciuca, and Maisin. The authors emphasized that the bacteriophage detected in organs was not produced by organ-induced bacterial modification as Bordet’s theory might suggest, since control experiments with normal organs or organs from bacteriophage-fed animals never yielded bacteriophage in cultures of susceptible bacteria.
Translation by Claude.ai:
Our research on the therapeutic value of bacteriophage has led us to examine the question of its fate in the organism.
We first investigated whether the bacteriophage supplied to the animal by the digestive route is absorbed. For this purpose, we give guinea pigs and mice the lytic filtrate in question, mixed with bread, and we examine the feces and organs of these animals.
The feces are added to broth, supplemented with a crystal of thymol. After 24 hours we take an ampoule of it, which we heat to 56° for one hour. We place two drops of the contents of this ampoule in a tube of broth, which we inoculate with the receptive microbe.
(Note from claude.ai: “’Réceptif’ (receptive) refers to a bacterial strain susceptible to the particular phage being tested, which is standard terminology for this period.”)
We observe that there is inhibition of growth in these tubes; which we attribute to the presence of bacteriophage and not to the trace of thymol. Indeed, if we heat the contents of this tube to 56° for one hour, to transfer a few drops into a new tube of broth, growth is still absent. According to our research, the bacteriophage principle is regularly found in the feces for several days; it remains there for a longer or shorter time depending on whether or not it finds microbes that it can influence (parasitize). This persistence, moreover, is perfectly explained when one takes into account its resistance to acids and to enzymes, which makes its destruction by digestive juices impossible. (1)
To search for the presence of bacteriophage in the organs, we sacrifice the animals and we aseptically remove the various organs, which we introduce into tubes of broth. If they remain sterile for 24 hours, we inoculate their contents with the receptive microbe, whose growth we monitor. In these media we detect no trace of bacteriophage. The result also remains negative when we add a few drops of the contents of the preceding tubes, heated to 56° for one hour, to broth. The bacteriophage principle therefore does not cross the intestinal mucosa; this fact is perhaps to be related to its inability to dialyze. (2)
As for the bacteriophage injected into animals, here is how we proceeded to determine its fate.
We inject variable doses of it into animals, which we sacrifice after a longer or shorter time, in order to remove the organs and to search in them for the presence of the lytic principle following the technique described above.
From the first hours following these injections, the bacteriophage is absorbed to pass into the blood, in accordance with the data of Bordet and Ciuca (3). However, its stay there is hardly long, for it is progressively eliminated from the organism, by the kidneys and the intestine, to the point of disappearing completely after 24 to 48 hours. The duration of stay varies somewhat with the inoculated dose, but after five days we have never found any trace of it. At this moment however, the spleen still contains notable quantities of it, as can be seen in the table below. This fact is to be related, it seems to us, to the role that this organ plays in infections, where…
(1) Depoorter and Maisin. Archives internationales de Pharmacodynamie et Thérapie, vol. XXV, fasc. V, VI.
(2) C. R. de la Soc. de biol., 26 January 1921.
(3) C. R. de la Soc. de biol., 29 January 1921
…it also intervenes actively to retain the microbes. In the spleen, however, the bacteriophage does not persist, given that fifteen days later, it is completely devoid of it. At this moment, the disappearance results, in our opinion, from the neutralization brought about by the antibacteriophage that forms in the organism, as shown by the experiments of Bordet, Ciuca and Maisin.
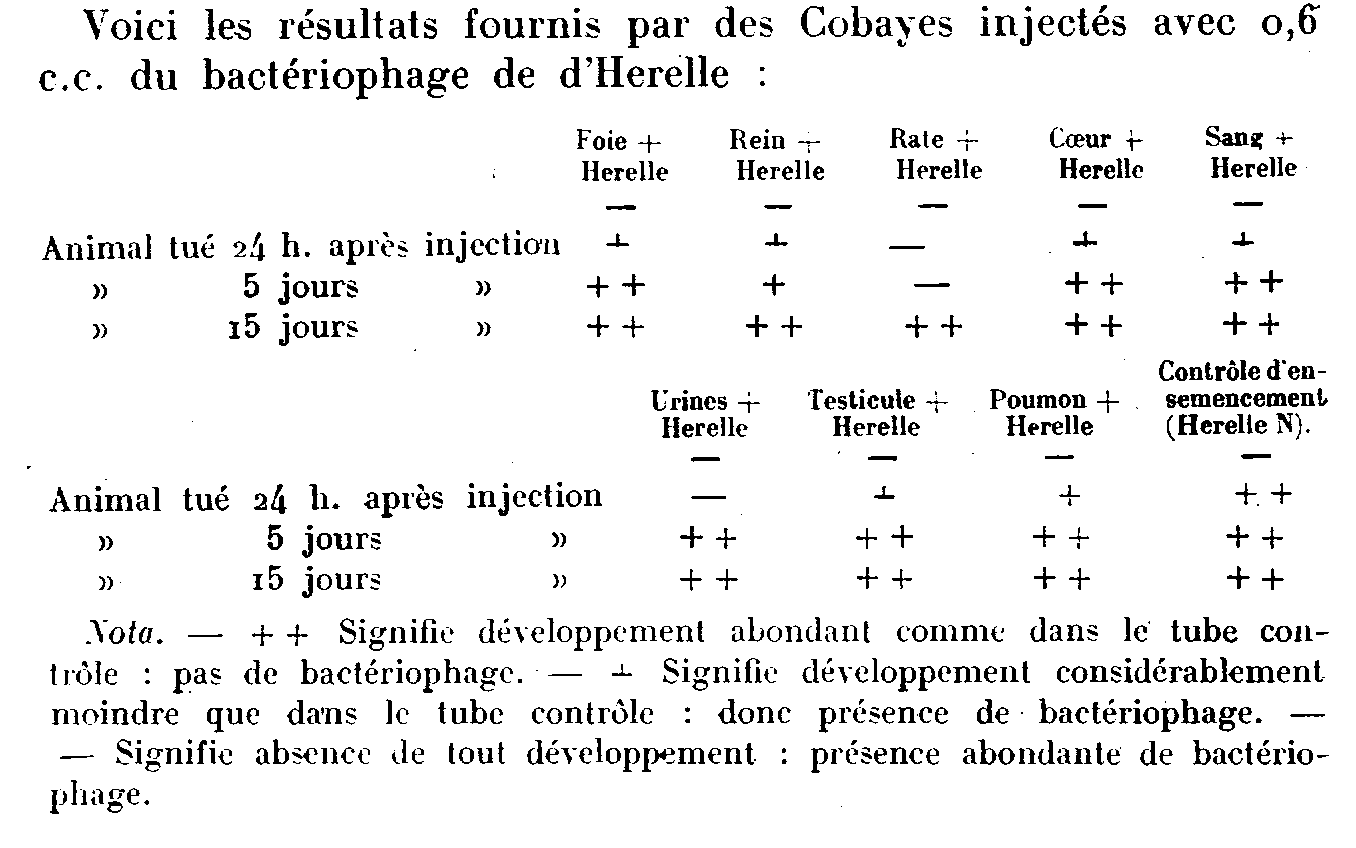
Here are the results provided by guinea pigs injected with 0.6 c.c. of d’Herelle’s bacteriophage: [see table image below]
[Table footnote:] Note. – + + Signifies abundant growth as in the control tube: no bacteriophage. – + Signifies considerably less growth than in the control tube: therefore presence of bacteriophage. – Signifies absence of all growth: abundant presence of bacteriophage.
We wish to point out that the bacteriophage that we thus find in the organs is not the product of a modification operated by these organs on the microbe to make it, in accordance with Bordet’s theory, capable of secreting the ferment in question; for this principle was always absent in the tubes of broth, where the microbes receptive to the bacteriophage had undergone contact with normal organs or with organs of animals fed with bacteriophage.
Conclusions: The bacteriophage is not absorbed under normal conditions by the digestive route.
When injected, it passes rapidly into the blood to be eliminated in the urine and feces.
It persists however in the spleen, until the moment when one can admit that the antibacteriophages intervene, to neutralize and destroy it there.
Possible Precedence as suggested by Claude.ai:
[Note: This assessment of precedence is based on the document itself and may not reflect comprehensive historical research.]
This article appears to be an important early systematic study of bacteriophage pharmacokinetics and biodistribution – essentially asking “what happens to phage when you put it in an animal body?” This was a critical question for the therapeutic use of bacteriophage, which was being actively explored in the early 1920s.
Several aspects suggest precedence or importance:
Oral vs. Injectable Routes: The finding that orally administered phage does NOT cross the intestinal barrier was significant for therapeutic applications. This would have important implications for how phage therapy should be administered.
First Detailed Tracking Study: While the authors cite Bordet and Ciuca (1921) for the observation that injected phage enters the blood, Appelmans appears to provide the first detailed tracking of phage through multiple organs over time, including the kinetics of elimination.
Splenic Sequestration: The observation that the spleen retains phage longer than other organs was novel and connected phage behavior to the spleen’s known immunological functions.
Antibody Neutralization: Linking the disappearance of phage from the spleen to antibacteriophage (neutralizing antibodies) helped establish that the immune system recognizes and responds to phage as foreign material.
The dates are telling: the references are from January 1921, suggesting this work was conducted very shortly after (or contemporaneously with) Bordet’s group’s initial observations. Given that Félix d’Herelle only clearly described bacteriophage in 1917, this 1921 work represents research within just a few years of phage discovery, making it part of the foundational literature on phage biology and a key early study informing phage therapy attempts.
OCR Work and Resulting Translation:
Our research on the therapeutic value of bacteriophage has led us to examine the question of its fate in the organism.
We first investigated whether the bacteriophage supplied to the animal by the digestive route is absorbed. For this purpose, we give guinea pigs and mice the lytic filtrate in question, mixed with bread, and we examine the feces and organs of these animals.
The feces are added to broth, supplemented with a crystal of thymol. After 24 hours we take an ampoule of it, which we heat to 56° for one hour. We place two drops of the contents of this ampoule in a tube of broth, which we inoculate with the receptive microbe.
(Note from claude.ai: “’Réceptif’ (receptive) refers to a bacterial strain susceptible to the particular phage being tested, which is standard terminology for this period.”)
LE BACTÉRIOPHAGE DANS L’ORGANISME.
Note de R. Appelmans, présentée par R. Bruynoghe.
Nos recherches sur la valeur thérapeutique du bacteriophage nous ont amené à examiner la question de son sort dans l’organisme.
Nous avons recherché d’abord si le bactériophage fourni à l’animal par voie digestive se résorbe. A cet effet, nous donnons à des Cobayes et des Souris, le filtrate lytique en question, mélangé à du pain et nous examinons les selles et les organes de ces animaux.
Les selles sont ajoutées à du bouillon, additionné d’un cristal de thymol. Après 24 heures nous en prélevons une ampoule, que nous chauffons à 56° pendant une heure. Nous mettons deux goutttes du contenu de cette ampoule dans un tube de bouillon, que nous ensemençons avec le microbe réceptif.
We observe that there is inhibition of growth in these tubes; which we attribute to the presence of bacteriophage and not to the trace of thymol. Indeed, if we heat the contents of this tube to 56° for one hour, to transfer a few drops into a new tube of broth, growth is still absent. According to our research, the bacteriophage principle is regularly found in the feces for several days; it remains there for a longer or shorter time depending on whether or not it finds microbes that it can influence (parasitize). This persistence, moreover, is perfectly explained when one takes into account its resistance to acids and to enzymes, which makes its destruction by digestive juices impossible. (1)
Nous constatons qu’il y a inhibition du développement dans ces tubes ; ce que nous attribuons à la presence de bacteriophage et non à la trace de thymol. En effet, si nous chauffons le contenu de ce tube à 56° pendant une heure, pour en porter quelques gouttes dans un nouveau tube de bouillon, le développement y fait encore défaut. D’après nos recherches le principe bactériophage se retrouve régulièrement dans les selles durant quelques jours ; il y reste plus ou moins longtemps suivant qu’il y trouve ou non des microbes qu’il peut influencer (parasiter). Cette persistance d’ailleurs s’explique parfaitement, quand on tient compte de sa résistance aux acides et aux ferments, qui rend sa destruction par les sucs digestifs impossible. (2)
To search for the presence of bacteriophage in the organs, we sacrifice the animals and we aseptically remove the various organs, which we introduce into tubes of broth. If they remain sterile for 24 hours, we inoculate their contents with the receptive microbe, whose growth we monitor. In these media we detect no trace of bacteriophage. The result also remains negative when we add a few drops of the contents of the preceding tubes, heated to 56° for one hour, to broth. The bacteriophage principle therefore does not cross the intestinal mucosa; this fact is perhaps to be related to its inability to dialyze. (2)
(Note from claude.ai: “The reference to dialysis at the end refers to the inability of bacteriophage particles to pass through dialysis membranes, which was an important observation about their physical properties in early phage research.”)
Pour rechercher la présence du bactériophage dans les organes, nous sacrifions les animaux et nous prélevons aseptiquement les divers organes, que nous introduisons dans les tubes de bouillon. S’ils restent stériles pendant 24 heures, nous ensemençons leur contenu avec le microbe réceptif, dont nous surveillons le développement. Dans ces milieux nous ne décelons pas trace de bactériophage. Le résultat reste également négatif, quand nous ajoutons quelques gouttes du contenu des tubes précédents, chauffés à 56° pendant une heure, à du bouillon. Le principe bactériophage ne franchit donc pas la muqueuse intestinale ; ce fait est peut-être à rapprocher de son inaptitude à la dialyse. (2)
As for the bacteriophage injected into animals, here is how we proceeded to determine its fate.
Quant aux bactériophage injecté aux animaux, voici comment nous avons procédé pour en déterminer le sort.
We inject variable doses of it into animals, which we sacrifice after a longer or shorter time, in order to remove the organs and to search in them for the presence of the lytic principle following the technique described above.
Nous en injectons des doses variables à des animaux, que nous sacrifions après un temps plus ou moins long, afin de prélever les organes et d’y rechercher la présence du principe lytique suivant la technique exposée plus haut.
From the first hours following these injections, the bacteriophage is absorbed to pass into the blood, in accordance with the data of Bordet and Ciuca (3). However, its stay there is hardly long, for it is progressively eliminated from the organism, by the kidneys and the intestine, to the point of disappearing completely after 24 to 48 hours. The duration of stay varies somewhat with the inoculated dose, but after five days we have never found any trace of it. At this moment however, the spleen still contains notable quantities of it, as can be seen in the table below. This fact is to be related, it seems to us, to the role that this organ plays in infections, where…
(1) Depoorter and Maisin. Archives internationales de Pharmacodynamie et Thérapie, vol. XXV, fasc. V, VI.
(2) C. R. de la Soc. de biol., 26 January 1921.
(3) C. R. de la Soc. de biol., 29 January 1921
Dès les premières heures qui suivent ces injections, le bacteriophage se résorbe pour passer dans le sang, conformément aux données de Bordet et Ciuca (3). Toutefois son séjour n’y est guère long, car il s’élimine progressivement de l’organisme, par les reins et l’intestin, au point de disparaître complètement au bout de 24 à 48 heures. La durée du séjour est quelque peu variable avec la dose inoculée, mais après cinq jours nous n’en avons plus jamais trouvé trace. A ce moment toutefois, la rate en contient encore des quantités notables, ainsi qu’on peut le voir dans le tableau ci-dessous. Ce fait est à rapprocher, nous semble-t-il, du rôle que cet organe joue dans les infections, où…
(1) Depoorler el Maisin. Archives internationales de Pharmacodynamie et Thérapie, vol. XXV, fase. V, VI.
(2) C. R. de la Soc. de bioi’.,26 janvier 1921.
(3) C. R. de la Soc. de biol., 29 janvier 1921
…it also intervenes actively to retain the microbes. In the spleen, however, the bacteriophage does not persist, given that fifteen days later, it is completely devoid of it. At this moment, the disappearance results, in our opinion, from the neutralization brought about by the antibacteriophage that forms in the organism, as shown by the experiments of Bordet, Ciuca and Maisin.
…il intervient également activement pour retenir les microbes. Dans la rate le bactériophage ne persiste toutefois pas, étant donné que quinze jours après, elle en est tout à fait dépourvue. A ce moment, la disparition résulte à notre avis, de la neutralisation opérée par l’antibactériophage qui se forme dans l’organisme, ainsi qu’il résulte des expériences de Bordet, Ciuca et Maisin.
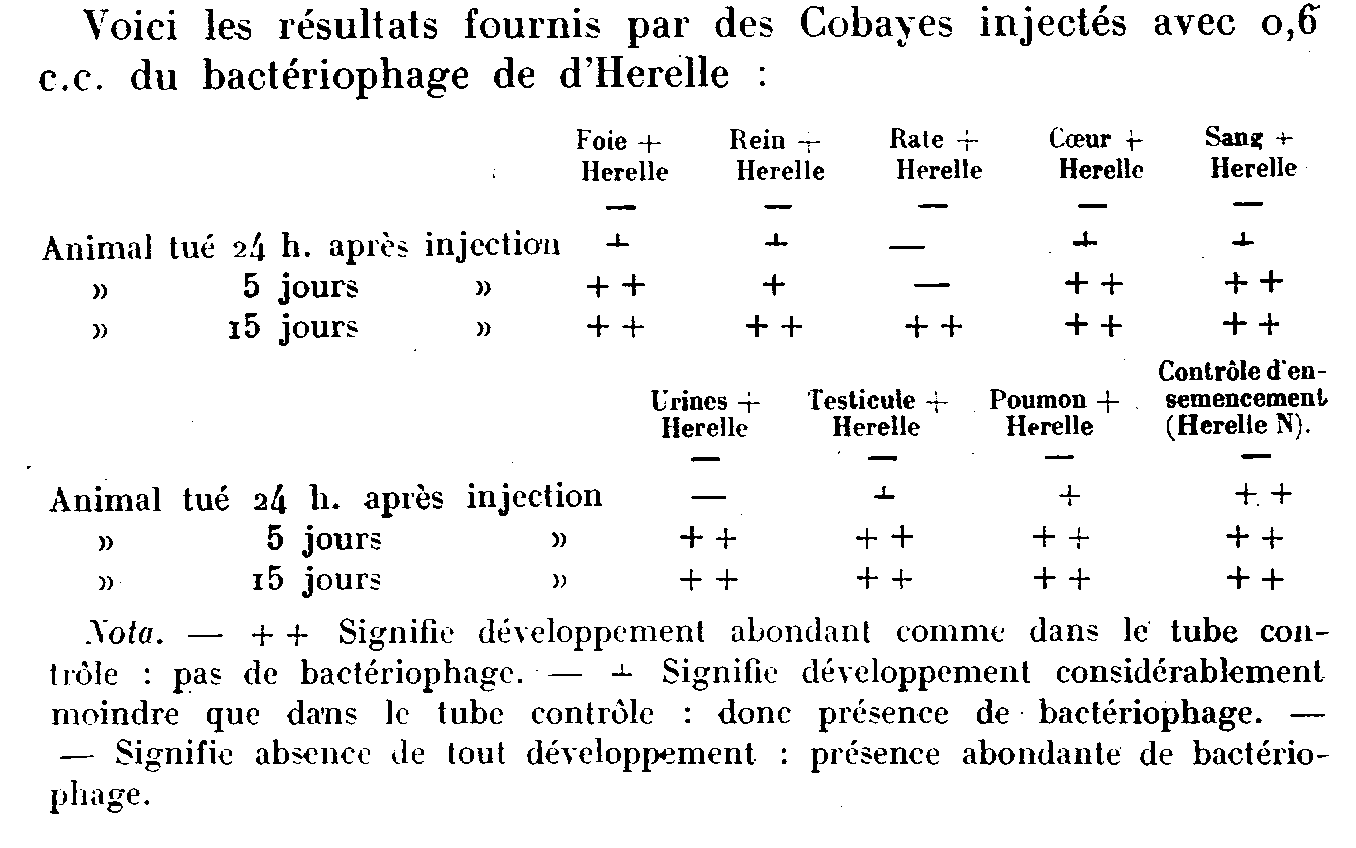
Here are the results provided by guinea pigs injected with 0.6 c.c. of d’Herelle’s bacteriophage: [see table image below]
[Table footnote:] Note. – + + Signifies abundant growth as in the control tube: no bacteriophage. – + Signifies considerably less growth than in the control tube: therefore presence of bacteriophage. – Signifies absence of all growth: abundant presence of bacteriophage.
Voici les résultats fournis par des Cobayes injectés avec 0,6 c.c. du bactériophage de d’Herelle :
[These are words from the table:] Foie, Rein, Rale, Coeur, Sang, tué, Urines, Testicule, Poumon, Contrôle d’enemencement.
[This is the table’s footnote:] Nota. – + + Signifie développement abondant comme dans Ie tube Contrôle : pas de bactériophage. – + Signifie déyeloppement considérablement moindre que da’ns le tube contrôle : done présence de bactériophage. – Signifie absence de lout dévelopment : présence abondante de bactériophage.
We wish to point out that the bacteriophage that we thus find in the organs is not the product of a modification operated by these organs on the microbe to make it, in accordance with Bordet’s theory, capable of secreting the ferment in question; for this principle was always absent in the tubes of broth, where the microbes receptive to the bacteriophage had undergone contact with normal organs or with organs of animals fed with bacteriophage.
Conclusions: The bacteriophage is not absorbed under normal conditions by the digestive route.
When injected, it passes rapidly into the blood to be eliminated in the urine and feces.
It persists however in the spleen, until the moment when one can admit that the antibacteriophages intervene, to neutralize and destroy it there.
Nous tenons à faire remarquer que le bactériophage que nous trouvons ainsi dans les organes, n’est pas le produit d’une modification opérée pas ces organes sur le microbe pour le rendre, conformément à la théorie de Bordet, apte à secréter le ferment en question ; car ce principe faisait toujours défaut dans les tubes de bouillon, où les microbes réceptifs. au bacteriophage avaient subi le contact d’organes normaux ou d’organes d’animaux nourris avec du bactériophage.
Conclusions : Le bactériophage ne se résorbe pas dans les conditions normales par voie digestive.
Injecté, il passe rapidement dans le sang pour s’éliminer dans l’urine et les selles.
Il persiste toutefois dans la rate, jusqu’au moment où on peut admettre que les antibactériophages interviennent, pour l’y neutraliser et l’y détruire.
In a Preliminary Note [Comptes rendus, t. 165, 1917, p. 373] I described a filtering microbe found in the excreta of convalescents from bacillary dysentery. The use of a technique less perfect than the one I had used at first [Comptes rendus du la SociétédeBiologie, séance du 7 décembre 1918] combined with the systematic examination of the stools of thirty-four patients, all suffering from dysentery due to Shiga bacilli, and several of whom could be followed daily from the beginning of the illness until the end of convalescence, allowed me to study in a more complete manner the mode of action of the bacteriophage microbe and to specify its role in the evolution of the disease.
In cases of bacillary dysentery, even very serious ones, but in which the patient’s condition improves rapidly, the bacteriophage microbe manifests its presence in a very active manner from the outset, both on cultures of the bacillus isolated from the patient’s excrement and on laboratory Shiga strains, from the moment when the symptoms begin to improve. The bacteriophage power with respect to the dysentery bacillus abruptly ceases to be detectable at the beginning of convalescence. From this moment on, repeated examinations also show the absence of pathogenic bacilli.
In cases where the disease is prolonged, the bacteriophage microbe shows only a nonexistent or slightly marked action, as long as the patient’s condition remains stationary. If, in some cases, the bactericidal action is relatively high on strains which have undergone numerous passages on culture media, on the other hand, it is always inappreciable or very weak on cultures of the bacillus coming from the patient under observation. The improvement is manifested as soon as the bacteriophage action becomes energetic with respect to the latter.
In long-term and relapsing forms, the bacteriophage power of the filtering microbe may, at certain times, be very energetic with respect to cultured bacilli and variable from one day to the next, although always relatively weak, with respect to the patient’s bacillus. Recovery closely follows the moment when the action of the bacteriophage microbe manifests itself in an equally intense manner for both strains. This action persists, with fluctuations in activity, as long as the patient remains a carrier of germs. This latter fact would even be likely to facilitate the detection of germ carriers, the detection of the bacteriophage microbe being simpler and more reliable than the search for the pathogenic bacillus in the stools.
I was able to verify that the action of the bacteriophage microbe was preponderant, not only with regard to the disappearance of the dysentery bacillus from the intestine once the disease had declared itself, but also during its outbreak. During the recent epidemic, I had the opportunity to observe several extremely mild cases in which the symptoms were limited to a few sputum and two or three diarrheal stools: now, in all these cases, the bacteriophage microbe was, from the beginning, present and endowed with a high antagonistic power. Despite the benignity of the affection, it was indeed dysentery because, in three of these cases, I was able to isolate from the first diarrheal stool emitted a typical Shiga bacillus.
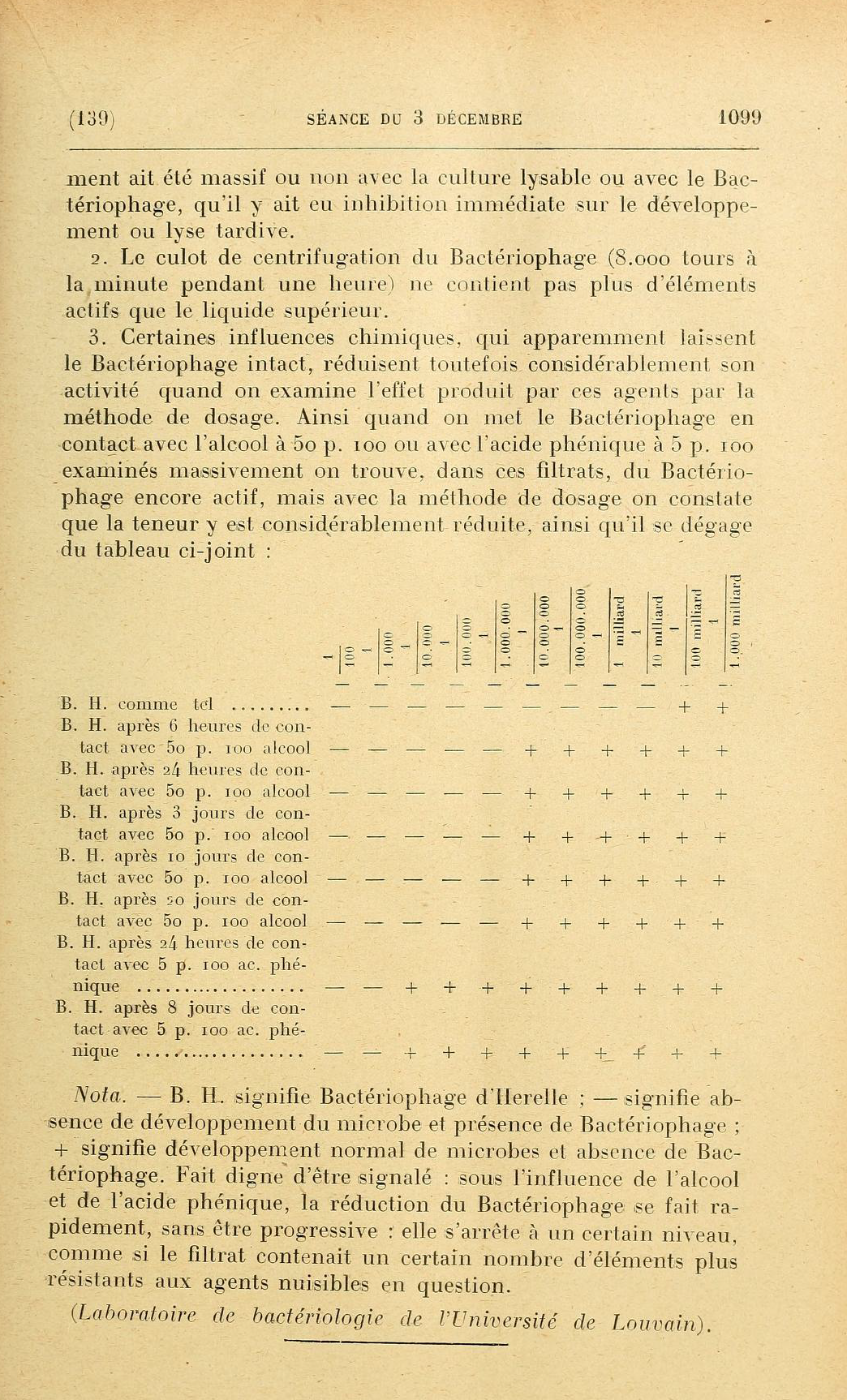
The bacteriophage microbe pre-exists in the intestine where it normally lives at the expense of B. coli. In normal stools, its antagonistic power towards the latter bacillus is always very weak; it can become considerable in various morbid states, in certain forms of enteritis and common diarrhea, for example. The presence of dysenteric bacilli in the intestine first determines a considerable exaltation of the virulence of the bacteriophage microbe towards B. coli, then, by a more or less rapid habituation, this virulence is exalted towards the dysenteric bacillus; it immediately or gradually reaches a considerable power leading to the rapid or gradual disappearance of the pathogenic bacillus. If the virulence of the bacteriophage microbe is immediately exalted [“very active”?], the dysenteric bacilli are destroyed from the start of their culture in the intestinal contents, the disease aborts before any symptoms or is limited to a few temporary disorders. If, for a cause which remains to be determined, the virulence of the bacteriophage microbe with respect to the pathogenic microbe does not manifest itself immediately or only manifests itself weakly, a fight is established between the two organisms, the dysentery bacilli multiply in the intestinal contents, infiltrate the mucous membrane, the disease breaks out and the patient’s condition then faithfully records the fluctuations in the fight. In summary, the pathogenesis and pathology of bacillary dysentery are dominated by two opposing factors: the dysentery bacillus, the pathogenic agent, and the filtering microbe bacteriophage, the agent of immunity. As a corollary, the experiment on the rabbit shows that cultures of the bacteriophage microbe have a preventive and curative power in the experimental disease; on the other hand, the bacteriophage microbe is invariably present in the intestine of the sick as soon as the symptoms improve; it therefore seems logical to propose, as a treatment for bacillary dysentery, the administration, as soon as the first symptoms appear, of active cultures of the bacteriophage microbe.
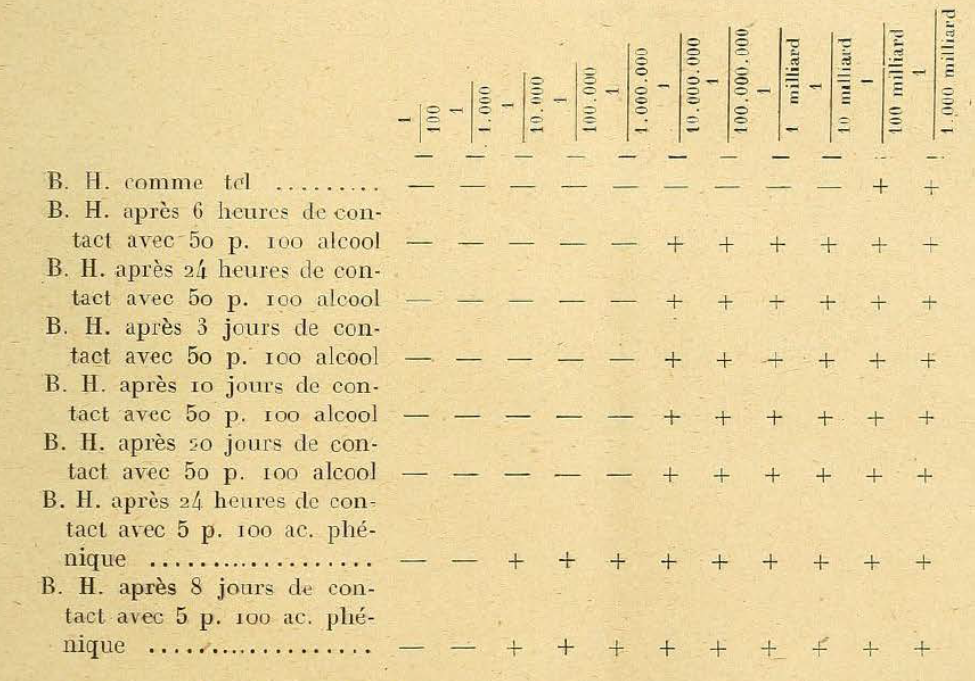
¶ In a note published in the Society of Biology on November 19, 1919, d’Hérelle indicated a method for measuring Bacteriophage. He puts 1/50,000 teaspoon of Bacteriophage into 10 c.c. of an emulsion containing approximately 250 million microbes per teaspoon and spreads a scoop of this mixture (i.e. 1/100 c.c.) onto a slanted agar tube. He then counts the number of dissolution areas and estimates from this the number of ultramicrobes. In fact, the Bacteriophage does not act like a liquid, exerting the same action over the entire seeding surface; lysis only occurs at locations where an ultramicrobe has been deposited on the agar.
¶ This method is, however, rather difficult to carry out because the clarification ranges [plaques?] can be extremely small and therefore not very apparent. Let us add to this that, when they are somewhat large, we could suppose that some of them result from a lack of seeding at this level [I’m unsure what this means].
¶ For the dosage, we tried the process of successive dilutions recommended by Miquel for water analysis. For this purpose we introduce, into tubes seeded with the microbe capable of undergoing lysis, decreasing quantities of Bacteriophage 1/10, 1/100, 1/1000, up to 1/1,000,000,000,000 [that’s 1/1 trillion or 1/1012!], according to that the microbe has normal development or undergoes immediate or subsequent lysis we admit the presence or the absence of the Bacteriophage in question.
¶ When we dose the Bacteriophage coming from tubes, inoculated with the same number of drops of Bacteriophage and the same number of drops of culture, we constant on both sides the same drops of culture [this too is phrasing I struggle with], we note on both sides the same activity. However, it happens from time to time that a given dilution provides a negative seeding for Bacteriophage, while the dilution ten times stronger still contains some. This is explained quite well with the notion of Bacteriophage presuming a living being. We also observe similar facts in the counting of water germs using Miquel’s method.
¶ This technique allowed us to make the following observations:
¶ 1. The Bacteriophage introduced into broth inoculated with lysable microbes, increases quantitatively during the stay in the oven [I assume this is an oven incubator]. This increase is approximately the same for a Bacteriophage and a given culture, whether or not the seeding was massive with the lysable culture or with the Bacteriophage, whether there was immediate inhibition on development or late lysis.
¶ 2. The centrifugation pellet of the Bacteriophage (8,000 revolutions per minute for one hour) does not contain more active elements than the upper liquid.
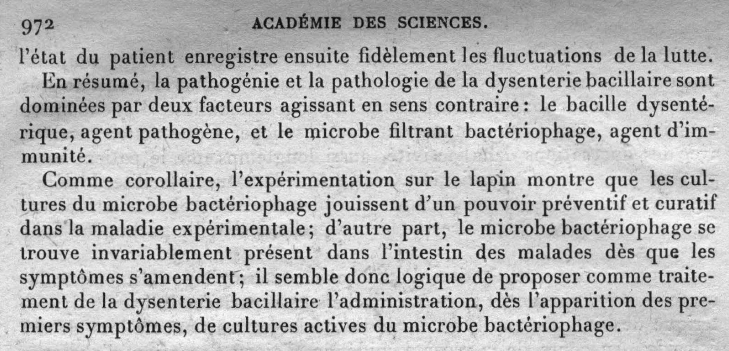
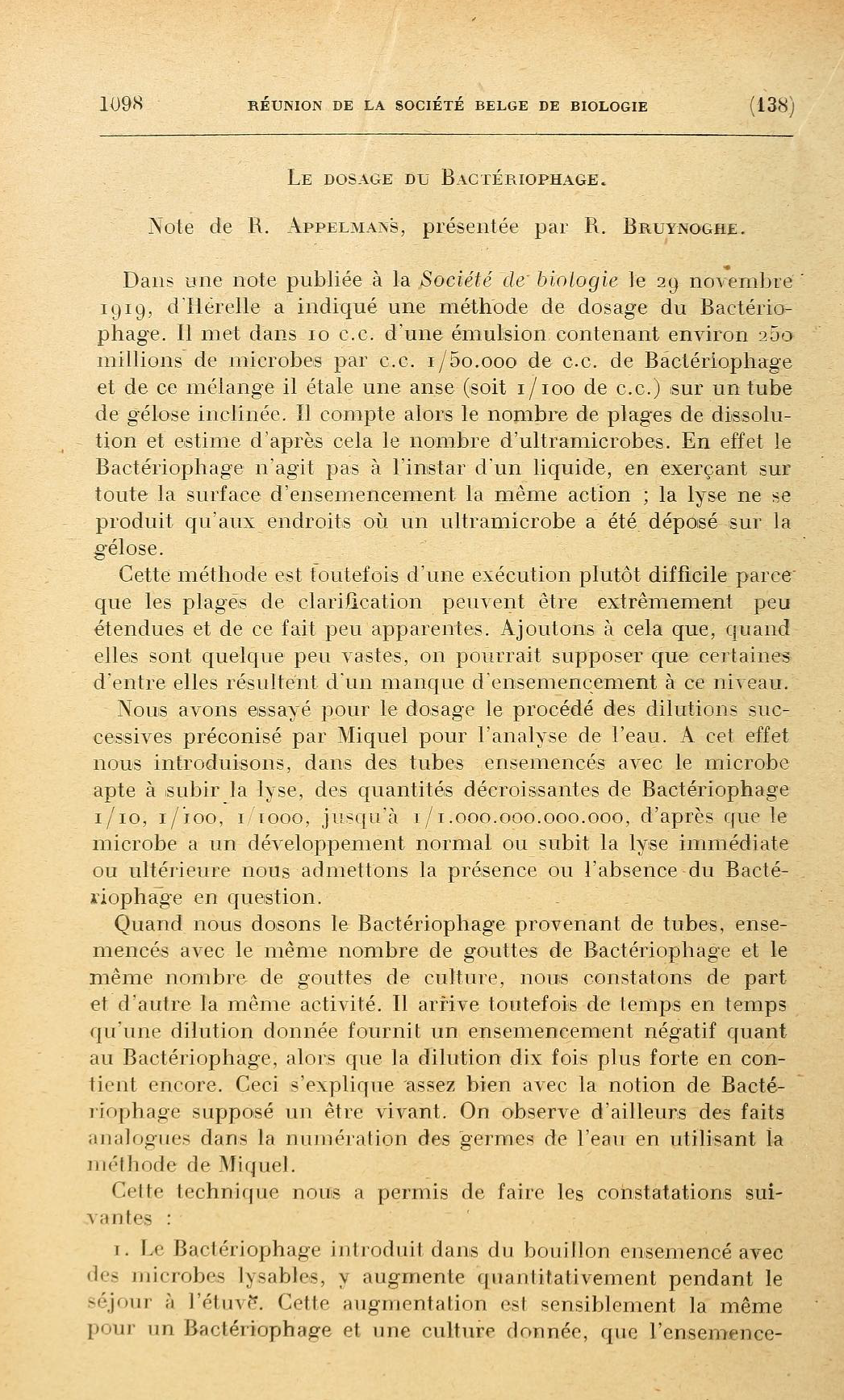
¶ 3. Certain chemical influences, which apparently leave the Bacteriophage intact, nevertheless considerably reduce its activity when the effect produced by these agents is examined by the dosage method. So when we put the Bacteriophage in contact with alcohol at 50 p. 100 or with 5 p. carbolic acid. 100 reviews massively we find [I don’t understand this phrasing]. In these filtrates, Bacteriophage is still active, but with the dosage method we see that the content is considerably reduced, as can be seen from the attached table:
¶ Note. — B. H. means Bacteriophage d’Herelle; — means absence of development of the microbe and presence of Bacteriophage; + means normal development of microbes and absence of Bacteriophage. Fact worthy of being noted: under the influence of alcohol and carbolic acid, the reduction of Bacteriophage occurs quickly, without being progressive: it stops at a certain level, as if the filtrate contained a certain number of elements more resistant to the harmful agents in question.
¶ (Bacteriology Laboratory of the University of Louvain).
An important question for those with ecological and evolutionary biological interests is when a given situation is of ecological relevance vs. when it might be more of evolutionary biological importance (Abedon, 2022b). Telling the difference can be important for all of us.
Ecology by definition is the interaction of organisms with their environments.
We can describe phage use as antibacterial agents, that is, phage therapy, as an example of community ecology, or more precisely an applied community ecology. This is community ecology because there is more than one species of organism involved, i.e., as making up an ecological community. Minimally this is the phage (species #1) and the targeted bacterium (species #2), but also of importance is the treated body (species #3).
By definition, bacterial resistance to phages is ecological, as it describes a specific type of interaction, in this case between at least two species, the phage and the bacterium. That the resistance ‘interaction’ is one of ‘non-‘ or ‘less-‘ contact by the bacterium with the phage antagonist is only a detail, just so long as this lack of interaction is phenotypic, i.e., as opposed to the phage and bacterium instead just happening to exist in different places.
Bacterial resistance to phages also of course can have evolutionary aspects.
Evolution by definition is a change in allele frequencies in at least one species, or, more precisely, changes in allele frequencies in one population, in either case as observed over time.
Often the changes in allele frequency that we care most about are consequences of the impact of natural selection, and natural selection under most circumstances has a strong ecological component. Indeed, natural selection in most cases can be defined as the impact of ecology on evolutionary biology (and hence, as an aside, the existence of the science of evolutionary ecology).
By definition yet again, changes in the frequency of phage-resistance alleles within a bacterial population is an evolutionary process and typically these changes are a consequence of natural selection. The selective agent would be that phage population that is negatively affecting a bacterial population, resulting in increases in the frequency of whatever bacterial alleles are conferring protection from this phage.
Of interest to phage therapy is that this ecology driving evolutionary biology can in turn drive ecology. Specifically, once the frequency of alleles conferring phage resistance are high enough within a targeted bacterial population, then the applied community ecology of phage therapy can be affected, e.g., phage therapy can stop working.
In addition, if the frequency of a phage-resisting allele is found to be 100% within the bacterial population, following phage treatment (i.e., a frequency of 1.0), then if nothing else this is indicative that bacterial survival – an ecological issue – in this instance likely is a function of the occurrence of phage resistance.
If the frequency of phage resistance instead is 0% following phage treatment (0.0), then if nothing else this is indicative that bacterial survival (again, an ecological issue) was not a function of the occurrence of phage resistance. In fact, any frequency of phage resistance below 100% within a targeted bacterial population means that phage-sensitive bacteria are persisting despite phage treatment. For an example of the latter, see, e.g., Box 2 of Abedon (2022c).
Phage-resistant bacteria may display reduced virulence against bodies or may be subsequently treated with a different phage. Consequently, in some ways phage-resistant bacteria are not necessarily that big of a deal as a midpoint of a phage treatment, and this can be particularly if a diversity of other treatment phages are available. Phage resistance is not desired nor welcome, of course, but evolution of phage resistance also is not a certain indication of phage therapy microbiological failure.
That, by the way, to a degree contrasts with the evolution of antibiotic resistance that can occur over the course of antibiotic treatments, which can indeed be associated with treatment failures with high likelihood. One difference is something called antagonistic pleiotropy – not to be confused with antagonistic coevolution (Abedon, 2022a)!!! – i.e., whether or not resistance alleles are otherwise costly to the carrying organism (Abedon, 2022d). If resistance is both easily attained and not ecologically costly, then, well, that can be problematic, particularly given only mono therapies. Another difference is the sheer abundance of diverse, typically safe-to-use phages that often can be available to phage therapists (Abedon and Thomas-Abedon, 2010).
In any case, the persistence of phage-sensitive bacteria despite phage treatment probably means that, for whatever reason, treatment phages are not able to successful infect targeted bacteria despite those bacteria being phage sensitive; again, see Box 2 of Abedon (2022c). This frankly should be viewed as a big deal as essentially by definition it implies a phage therapy microbiological failure, one that may or may not be easily rectified, or at least a lack of complete eradication of phage-sensitive bacteria. I mean, how does one deal with phages not being able to easily reach and/or kill the otherwise phage-sensitive bacteria they are targeting?
Perhaps, as an answer to that question, some other phage that happens to be able to do a better job of reaching and/or killing those otherwise phage-sensitive bacteria might be available for use. That certainly is possible, but at this point in time we really aren’t all that good at figuring out what might constitute a better phage for phage therapy, other than in terms of host range – though see for example Bull et al. (2002; 2019) – and particularly better than the phage that we started with, presumably assuming that the first phage tried we thought was the better phage for phage therapy, hence why it was used first.
Of course, we almost take it as a matter of faith that phage carriage of extracellular polymeric substance (EPS) depolymerases (Danis-Wlodarczyk et al., 2021b) will solve many problems of phage penetration to targeted bacteria. But whether that is actually true in all instances, e.g., such as phage distribution throughout lungs – yet again, see Box 2 of Abedon (2022c) – is in my opinion just not known.
How might use of a phage cocktail instead result in complete eradication of a phage sensitive bacteria when a monophage does not? Just better odds that at least one of the phages used will be particularly good at achieving this? As another aside (Danis-Wlodarczyk et al., 2021a; Abedon, 2022c), note that it can be helpful to just apply a phage or phages at higher or multiple doses before giving up on a given treatment strategy!
At any rate, not being able to eradicate bacteria from an infection even though those bacteria are sensitive to a given treatment can be a far greater problem than failure that get rid of bacteria that explicitly are not susceptible to a treatment protocol. That is, there exits a basic problem in the applied ecology of treatments if not even phage-sensitive bacteria can be removed in full, just as there is a basic problem for an antibiotic treatment if the antibiotic is unable to fully eliminate even antibiotic-sensitive bacteria, a.k.a., the concept of antibiotic tolerance. For a bit on the latter, see Appendix A1 of in fact yet yet again, Abedon (2022c).
So where exactly am I going with this? At the end of a phage treatment, it is important to know whether the frequency of phage-resistant bacteria among the targeted bacterial population is high (at or approaching 100%) rather than low (near 0%). But high precision in that measurement, e.g., more than just whole percentage-point differences, really is not all that important. Why not?
Especially ecologically, there likely is little difference between 0.1%, 0.01%, or even maybe 10% or 50% of the bacteria being phage resistant, as that will still leave an awful lot of phage-sensitive bacteria having escaped phages during treatment. At some probably higher frequency of phage resistance we might come to feel that the frequency of remaining phage-sensitive bacteria is less important, but exactly where that point lies is difficult to say. My gut feeling, though, is that at the point where we start having to do statistics to tell the difference, i.e., at a point where higher precision in measurements becomes important, the importance of differences in the frequencies of phage-resistant bacteria – 100% or a tiny bit less than 100% – probably are no longer all that relevant. (For consideration of the statistics of plating-based enumeration, see Abedon and Katsaounis, 2021.)
Ah, you are saying, clearly therefore I am leading up to claiming that if we are interested instead in the evolutionary biology phage resistance, then in that case we really should care about measuring resistance frequencies with higher precision. And you would be absolutely right! Except also maybe not.
The problem here is that a key word in the definition of evolution that we are using is “Change”, and by definition change cannot be measured using only a single data point, or in the case of quantifying evolutionary change, a single time point. Thus, no matter how precisely you measure the endpoint frequency of phage-resistant bacteria, that will not tell you that evolution has occurred in the course of phage therapy treatment, much less how much evolution.
Here is the basis of this latter point: At the start of an experiment, if your population of bacteria ever is going to contain phage-resistant members, then it likely already does contain those mutants (this, by the way, is why only-qualitative determinations that phage resistance is present, e.g., such as following phage treatments, are basically meaningless). Exceptional would be if the starting number of bacteria involved is so low that this number is, e.g., less than the inverse of the rate of mutation to phage resistance. Thus, for every time a bacterium divides, let’s say that there is a probability of 10-5 that a mutation to phage-resistance will occur. If so, then in a population of 106 bacteria, on average 10 phage-resistant bacteria will be expected to be present, more or less (Abedon et al., 2021).
That last part, “More or less”, is crucial, however, as the frequency with which mutations conferring phage resistance are expected to be present is predicted to somewhat “Fluctuate” about an average (Luria and Delbrück, 1943). In practice, this means that even if you precisely know bacterial rates of mutation to resistance to a given phage, you still will not know how many phage-resistant bacterial mutants will be present prior to the start of treatments. (As yet another aside, actually calculating mutation rates, vs. just mutant frequencies, is a not trivial thing to do.)
Without knowing the frequency of phage resistance prior to the start of treatments, then you are only really guessing whether evolution has occurred in the course of a phage treatment, no matter how precisely frequencies of phage resistance may be measured after a treatment is done.
In short, ecologically, the precision of measures of frequencies of bacterial phage resistance need not be all that high to possess high value in understanding the outcome of phage treatments. I mean, either phage-sensitive bacteria have persisted despite prior treatments or they have not, without a need to describe percentages with precision past the decimal point. Thus, 50.0% vs. 50.1%? Who cares? Indeed, 50% vs. 51%, who cares?
Alternatively, if one really cares about being precise in monitoring the evolution of phage resistance, then the most important place to emphasize that precision actually should be prior to the start of treatments, i.e., prior to initial phage application, and only then should one be measuring frequencies of phage resistance after treatments as well. But don’t forget that you need to have this information for explicitly that bacterial culture that is being treated, since evolutionarily all we really will care about is how a specific bacterial culture as a population changes in allele frequencies over time, and in phage therapy that bacterial population is precisely the one that you are treating.
Even so, how much more than order-of-magnitude precision do we really need in monitoring the evolution of phage resistance during phage treatments? Will we really care for example if the frequency of phage-resistant bacteria have changed from 10-5 to 10-5.5? And how hard would we have to try to be sure that such a relatively small change is actually real? I mean, seriously, except for the most hard-core evolutionary experiments, who would really care?
For what it is worth, when I look at the outcome of a phage treatment, if all of the targeted bacteria remaining are phage resistant, then I know what went wrong (clue: the bacteria have evolved resistance to the treatment phages, i.e., an evolutionary outcome). But when I look at the outcome of a phage therapy experiment and a substantial portion of the bacteria remaining are still phage sensitive, then more often than not I can only speculate as to what might have gone wrong, except again for those bacteria that have evolved phage resistance (Abedon, 2022c). Still, this latter scenario should be viewed at least as an ecologically relevant outcome.
But bottom line: Obtaining an additional decimal place or two in describing the frequency of phage-resisting alleles within the treated bacterial population generally will not greatly aid in improving the precision of our applied ecological speculation.
Afterthought:
You would think that this essay came into existence as a natural outgrowth of the cited publications, particularly Abedon (2022c), but you would be wrong! On the other hand, I did wait a few months until that publication was published and available open access. Thanks for your interest!
Literature Cited:
Abedon, S. T. 2022a. A primer on phage-bacterium antagonistic coevolution, p. 293-315. In Bacteriophages as Drivers of Evolution: An Evolutionary Ecological Perspective. Springer, Cham, Switzerland. https://link.springer.com/chapter/10.1007/978-3-030-94309-7_25
Abedon, S. T. 2022b. Frequency-dependent selection in light of phage exposure, p. 275-292. In Bacteriophages as Drivers of Evolution: An Evolutionary Ecological Perspective. Springer, Cham, Switzerland. https://link.springer.com/chapter/10.1007/978-3-030-94309-7_24
Abedon, S. T., and T. I. Katsaounis. 2021. Detection of bacteriophages: statistical aspects of plaque assay, p. 539-560. In D. Harper, S. T. Abedon, B. H. Burrowes, and M. McConville (ed.), Bacteriophages: Biology, Technology, Therapy. Springer Nature Switzerland AG, New York City. https://link.springer.com/referenceworkentry/10.1007/978-3-319-40598-8_17-1
Abedon, S. T., K. M. Danis-Wlodarczyk, and D. J. Wozniak. 2021. Phage cocktail development for bacteriophage therapy: toward improving spectrum of activity breadth and depth. Pharmaceuticals 14:1019. https://pubmed.ncbi.nlm.nih.gov/34681243/
Bull, J. J., B. R. Levin, T. DeRouin, N. Walker, and C. A. Bloch. 2002. Dynamics of success and failure in phage and antibiotic therapy in experimental infections. BMC Microbiol. 2:35. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC138797/
Bull, J. J., B. R. Levin, and I. J. Molineux. 2019. Promises and pitfalls of in vivo evolution to improve phage therapy. Viruses 11:1083. https://pubmed.ncbi.nlm.nih.gov/31766537/
Danis-Wlodarczyk, K., K. Dabrowska, and S. T. Abedon. 2021a. Phage therapy: the pharmacology of antibacterial viruses. Curr. Issues Mol. Biol. 40:81-164. https://pubmed.ncbi.nlm.nih.gov/32503951/
Danis-Wlodarczyk, K. M., D. J. Wozniak, and S. T. Abedon. 2021b. Treating bacterial infections with bacteriophage-based enzybiotics: in vitro, in vivo and clinical application. Antibiotics 10:1497. https://pubmed.ncbi.nlm.nih.gov/34943709/
Luria, S. E., and M. Delbrück. 1943. Mutations of bacteria from virus sensitivity to virus resistance. Genetics 28:491-511. https://pubmed.ncbi.nlm.nih.gov/17247100/
With antimicrobial resistance a rising global crisis, western medicine’s interest is turning to phage therapy as an alternative to antibiotics. Challenging past uncertainty in phage therapy’s commercial viability, recent developments such as highly positive results of compassionate use cases in the US has excited the field and the next step is successful phase II clinical trials.
Phage Futures Congress is a translational phage therapy conference where Steffanie Strathdee, Tom Patterson, the FDA, and others will discuss how we move phage therapy forward in the US. A number of A Smaller Flea authors will be speaking or in attendance: Jessica Sacher of Phage Directory, Ben Chan of Yale Univeristy, Shawna McCallin of PhageForward. I am pleased to announce that I have also joined the Scientific Advisory Board for the congress
DuPont Nutrition & Health is a USD 4.7 billion global business and one of the world’s largest producers of specialty food ingredients, developing and manufacturing solutions for the global food & beverage, nutrition and pharma market. With more than 8,500 employees, 50+ manufacturing sites and 20+ R&D centres across the world, N&H is on a mission to make food safer, more sustainable, better tasting and more nutritious.
N&H is part of DowDuPont, a globally listed company, which came to life following the merger of Dow Chemical and DuPont in 2017. DowDuPont has a turnover of approximately $62 billion, employs around 98,000 FTEs and is headquartered in Wilmington, USA. The Upstream Culture Development group is part of the R&D Department of its Culture Development and Food Protection Division. The group is strongly involved in knowledge development and is responsible for selecting strains of microorganisms to be used in the design of starter cultures for dairy and other fermentation industries.
When Twitter told me last week that my former next-door lab neighbour just mailed phages to a dying girl, I actually started believing that my research might mean something. Not eventually, but today.
I used to think phage researchers like me were meant to do plaque assays in a lab for a few decades, while “other people out there, in 50 years, maybe” would sift through the information I would eventually publish and use it to cure people of bacterial infections. I’d gotten comfortable with the idea of doing research for the sake of research. I’d become proud of my patience and my willingness to do science without needing it to help people. I thought this made me a good scientist.
My thinking started to change when I heard the story of Tom Patterson, the patient cured last year in San Diego of his A. baumannii infection following phage therapy. The part that really got to me was how his treatment was essentially crowd-sourced in an effort led by his wife, Steffanie Strathdee (@chngin_the_wrld).
Fast forward to a week and a half ago, when I noticed that Steffanie’s phage-sourcing efforts were back in full force. This time, she was working to save 25-year-old Mallory Smith from drug-resistant B. cepacia. This time, however, I was watching it in real time. She used hashtags and @mentions to ask researchers to send phages. She used caps lock to emphasize urgency.
I had a fleeting thought about texting my friend from Jon Dennis’ lab at the University of Alberta, because I knew they worked on B. cepacia. Instead, I thought, those hashtags aren’t for grad students like me or for labs like ours. Those messages are for companies that make lots and lots of phages using proprietary processes, for labs with ties to hospitals that work with patients, for government organizations like the US Navy and its phage library.
And then I saw Steffanie tweet a thank-you to @JonDennis8 for sending phages, and I realized that the kind of researcher she was trying to reach was me.
I shared all of this with my friend Jan Zheng, who specializes in how humans interact with computers. He designs ways of simplifying this experience. Upon seeing the Twitter trail and hearing about Mallory and Tom’s stories and the phage hunts associated with both, he excitedly proclaimed that he knew how we could simplify this experience too.
We spent the next several days creating Phage Directory (phage.directory), a website designed to help treat patients infected by drug-resistant pathogens with safe and effective doses of phages, on a last-resort, emergency basis through the FDA’s Emergency Investigational New Drug process.
Although phage therapy is not yet ready to be adopted by mainstream Western medicine, the FDA is ready for phage therapy on a case-by-case basis as long as antibiotics are tried first. To paraphrase what Scott Stibitz of the FDA said at the Evergreen Phage Meeting this year: those of us who have been repeating the trope that the FDA is an enemy of phage therapy should stop, because we’re wrong.
A major part of what Jan and I envision that this directory will do is to serve as a searchable resource and alert service to help patient advocates find phage researchers who are willing to send phages to a patient in need, on an individual, on-demand basis. We also hope to connect these researchers with those willing to test the host range of these phages on patient isolates and then to propagate and purify promising candidates prior to shipment to the patient.
Two days into building Phage Directory, we found out that Mallory had passed away. This heart wrenching news spurred us on, and we launched the site last Friday. We made a Twitter account and began reaching out to phage researchers and others who might be interested in the cause.
Now, a week after its launch, we have reached 100 followers on Twitter (mostly phage biologists) and have been talking to Steffanie about how a directory like this would optimally function. She put us in touch with Tobi Nagel of Phages for Global Health, who was excited to talk with us. Phages for Human Applications Group Europe (P.H.A.G.E.) has encouraged its members to sign up, and several of them have. Sylvain Moineau and the Félix d’Hérelle Center at Université Laval in Canada are also on board.
On Monday of this week, we found out that Mallory’s parents were thrilled to hear about Phage Directory, and want to help us help other patients in honour of their daughter. On Tuesday, the journalist at STAT News who wrote the original article detailing Steffanie’s efforts to find phages for Mallory interviewed Jan and me for his next story.
What began as an offhand comment that we should make “PhageBook” has become a very real and impassioned effort to identify the barriers to treating patients with phages, particularly in the West, and to systematically design ways to overcome these barriers. Especially at this stage, we are open to suggestions on how best to put together this resource.
In addition to its role as a phage researcher directory and virtual phage library, we envision Phage Directory becoming a resource for physicians and other patient advocates seeking to learn about the actions required to initiate phage therapy in a patient, the associated legal implications, and the particular phages and treatment strategies available.
We see it becoming a communication platform that facilitates and organizes secure exchanges between doctors and researchers, before, during and after phage treatment, e.g. which phages should be tried first or next? How does susceptibility to each phage and antibiotic evolve over the course of each treatment iteration?
We see it providing the public with an interactive lens into the world of phage therapy, where patients and families can identify and communicate with phage researchers and physicians willing to facilitate phage therapy.
We see it helping to build legitimacy and transparency into the process of phage therapy to help regulatory agencies gain confidence in its feasibility.
Overall, we see Phage Directory as an action-oriented tool that will break down barriers to phage therapy by providing a multi-stakeholder communication platform designed to simplify and streamline the process.
Since I’ve joined our remarkable phage community, I’ve become increasingly conscious of its deep commitment to bringing phage therapy to modern medicine. I hope that many of you will add yourselves to Phage Directory and that you’ll sign up for the alert service so you can be contacted in the event that a patient needs your phages.
Finally, I hope that you’ll spread the word about this initiative so we can all take advantage of the momentum generated from Tom and Mallory’s recent public battles to put what we’ve collectively been writing and thinking about for years into a new kind of action.